Ultivit™ Kids (60)
Ultivit™ Kids contains natural beta-carotene, natural form of vitamin E, bioavailable forms of minerals, bioactive form of vitamin D, easily absorbed and safe form of iron (carbonyl iron).
Ultivit™ Kids does not contain yeast, wheat, milk, soy, starch, artificial colors, preservatives.
The product has been manufactured using high quality pure raw materials and the technology that ensures all their beneficial properties intact, in strict compliance with GMP and TÜV regulations.

What can be more important than you child’s health?
Does your kid receive adequate amount of vitamins and minerals every day?
Everyone knows that vitamins and minerals are essential for child’s proper growth and development. The researches show that nowadays lack of vitamins in children’s diet is not a seasonal phenomenon; they suffer from vitamin and mineral deficiencies all year round.
One of the reasons – unhealthy changes in our diets. Children also often prefer “tasty” to “good for you”.
Some children are quite fussy to take green leafy vegetables and fruits thus compromising their intake of micronutrients from dietary sources.
The full genetic potential of the child for physical growth and mental development may be compromised due to subclinical deficiencies of micronutrients which are commonly referred to as "hidden hunger".
Micronutrients are required for the integrity and optimal functioning of the immune system. Children with subclinical deficiency of micronutrients are more vulnerable to develop frequent and more severe common day-to-day infections thus triggering a vicious cycle of undernutrition and recurrent infections.
Micronutrients are required for optimal physical growth and neuromotor development.
The first 3 years of life are most crucial, and children are vulnerable to the hazards of undernutrition. All efforts should be made so that preschool children are given a balanced and nutritious home-based diet. However, it has been shown that it is not possible to meet 100% requirements of recommended dietary allowances (RDA’s) of micronutrients from dietary sources alone and most preschool children need administration of nutritional supplements to optimize their genetic potential for physical growth and mental development. (1)
Santegra®’s Ultivit™ Kids guarantees that your child will receive essential vitamins and minerals. The vitamins and minerals in Ultivit™ Kids are perfectly balanced. The chewable tablets taste great and the kids will never forget to take them daily.
Ultivit™ Kids contains:
Beta-carotene that the body converts into vitamin A, a potent antioxidant that defends cells from the damage caused by free radicals, improves vision.
Vitamin C is a powerful antioxidant, which is essential for immune system. Helps to increase body’s defense against infections. It is vital to the production of collagen, the "glue" that strengthens skin, bones, teeth, blood vessels, cartilage etc. Vitamin C plays vital role in the support of the cardiovascular system. Enhances iron absorption.
Vitamin D is important in building strong bones and teeth. Vitamin D plays an important role in calcium and phosphorus absorption.
Vitamin E is a potent antioxidant, which protects the body against free radicals.
B group vitamins are necessary for numerous essential functions in the body.
Iron is a key component in hemoglobin, the oxygen-carrying pigment in red blood cells, helps the blood supply oxygen to the body. Iron prevents iron deficiency anemia. It’s essential for the immune system and for promoting overall health. Lack of iron not only causes fatigue but can affect the learning ability.
Iodine is the thyroid gland component and the adequate iodine helps the body to get energy, fight excess weight; promotes alertness. Iodine is essential for healthy skin, nails and hair.
Manganese is an essential trace mineral needed for growing processes, healthy skin, bone and cartilage formation, blood formation, immune system.
Zinc stimulates the activity of about 200 enzymes. Among its many functions, zinc helps to maintain a healthy immune system, supports normal growth and development during childhood and adolescence.
Ultivit™ Kids does not contain yeast, wheat, milk, soy, starch, artificial colors, preservatives.
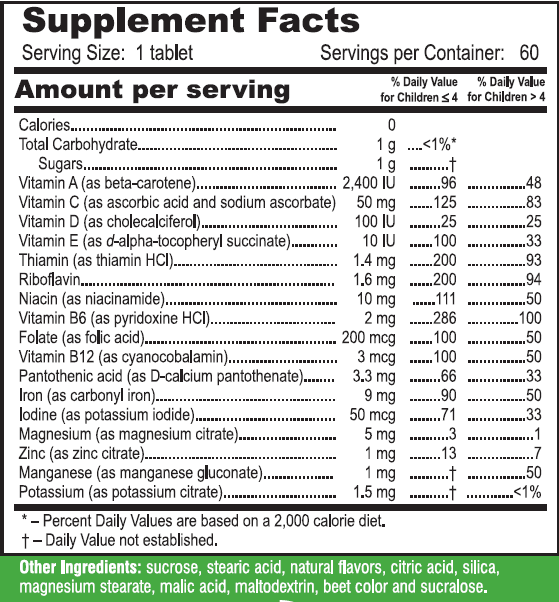
4-7 years old children take ½ tablet daily at mealtime, 7-12 years old children take 1 tablet daily at mealtime, children over 12 years take 2 tablets daily at mealtime.
Contraindication
Individual intolerance.
Keep out of the reach of children. In case of overdose seek immediate medical attention.
Vitamin and mineral deficiencies afflicts over two billion people worldwide. The highest prevalence is in regions where diets are poor and chronic hunger is widespread. Vitamin and mineral deficiency often has no visible warning signs. The effects, however, are devastating – resulting in decreased immune system functioning, impaired brain and physical development, preventable blindness, and severe birth defects.
The best way for the children to get essential vitamins and minerals is eating a variety of healthy foods. That means eating plenty of fresh fruits, vegetables, fish, lean meat, whole grains, nuts, legumes, and milk.
The problem is that children don't always eat the way we would like them to eat! Picky eaters might not get all the vitamins, minerals and other important nutrients they need.
Kids often prefer sweets, processed and junk food that do not contain much nutritional value, just unhealthy fats, sugar and calories.
Some experts believe that minerals are depleted in our soil, and therefore much of our produce may be deficient of minerals.
The report of the World Health Organization summarizes results from nutritional status studies undertaken in 80 countries and identifies four target nutrients crucial to health and development both in utero and in childhood: iron, vitamin A, iodine and folate.
Lack of vitamin A has left up to 40% of children less than 5 years old in the developing world with compromised immune systems, leading to the early deaths of one million young children every year.
Vitamin A deficiency affects 140 million preschool children. It weakens the immune system and increases vulnerability to different diseases. Vitamin A deficiency is the leading cause of child blindness in developing countries.
Folate deficiency results in about 200 000 severe birth defects annually. (2)
Iron deficiency causes iron deficiency anemia, impairs mental development in young children and results in a lowering of national intelligence quotients.
Iron deficiency affects two billion people worldwide — more than 60% are children ages 6-24 months – impeding cognitive development, causing poor learning and school performance.
Iodine deficiencies cause up to 20 million babies to be born with mental defects every year.
Iodine deficiency affects 780 million people worldwide. Every year, 20 million children are born mentally impaired because their mothers did not consume enough iodine while pregnant. It is the leading cause of preventable mental retardation.
Pediatricians have begun to look harder at Vitamin D levels in children because this vitamin, once thought to be primarily involved in calcium absorption, is now being shown to have significant implications for a variety of health conditions which manifest in later life. (3)
And while parents and doctors have assumed that children took in enough Vitamin D from sunshine exposure, supplemented foods, or vitamin supplements, a recent study has found that 12% of American infants and toddlers are deficient in vitamin D, and another 28% are at risk for it. (4)
Recent research has been showing Vitamin D has a potential impact on the development of some chronic diseases including heart disease, high blood pressure, diabetes mellitus, inflammatory and autoimmune diseases and cancer. (5)
Kids who do not eat enough fruits and vegetables are at risk of vitamin C deficiency. Vitamin C is important for the immune system, for the connective tissues, and protects from damaging free radicals.
The B complex vitamins work together synergistically to provide a number of benefits. B vitamins are involved with carbohydrate metabolism, serve to produce energy, help maintain the nervous system, are necessary for proper brain functioning.
Zinc deficiency is linked to nearly one million child deaths a year from diarrhea and pneumonia.
Vitamins and minerals are important elements of the total nutritional requirements of your child. Because the human body itself is unable to produce adequate amounts of many vitamins, they must be obtained from the diet.
Kids who don't get all the nutrition they need from their diets should take children's vitamins as a good way to ensure that they get enough vitamins and minerals.
OBJECTIVE: To compare the food consumption and nutrient intakes of German children and adolescents in the 1980s with present dietary habits.
DESIGN: Two cross-sectional representative surveys, the German National Food Consumption Study (Nationale Verzehrsstudie, NVS) from 1985-8 and the nutrition module 'EsKiMo' of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS) from 2006, were analyzed for differences in food and nutrient intakes stratified by age and sex groups.
SETTING: Secondary analyses of data from representative observational studies.
SUBJECTS: Children and adolescents aged 6-17 years living in Germany in the 1980s (n 2265) and in 2006 (n 2506).
RESULTS: Food consumption was characterized by higher amounts of vegetables/pulses, fruits/nuts and beverages and less meat products/sausages, butter, fats/oils, potatoes/potato products and bread/pastries in 2006 than in 1985-8. The overall changes in food intake were reflected in improvements of macronutrient composition, increased water intake and lower energy density of the diet.
Intake of most vitamins and minerals increased in relation to energy intake, but the nutrient density of the diet for vitamins B12 and D decreased.
The most critical nutrients observed in NVS and EsKiMo were folate, vitamin D, vitamin A, vitamin E, Ca and Fe. In addition, dietary fiber intake was relatively low and fatty acid and carbohydrate compositions were not favorable.
CONCLUSIONS: Further efforts will be necessary to improve dietary habits among children and adolescents. (6)
A recent UK-based study investigated whether daily supplementation with vitamins/minerals could modulate cognitive performance and mood in healthy children. In this investigation, eighty-one healthy children aged from 8 to 14 years underwent laboratory assessments of their cognitive performance and mood on the first and last days of 12 weeks' supplementation with a commercially available vitamins/mineral product.
The assessment was done at pre-dose, 1h and 3h post-dose. Interim assessments were also completed at home after 4 and 8 weeks at 3 h post-dose. Each assessment comprised completion of a cognitive battery, which included tasks assessing mood and the speed and accuracy of attention and aspects of memory (secondary, semantic and spatial working memory).
The vitamin/mineral group performed more accurately on two attention tasks: 'Arrows' choice reaction time task at 4 and 8 weeks; and 'Arrow Flankers' choice reaction time task at 4, 8 and 12 weeks. Picture Recognition errors showed significant decrement at 12 weeks.
While mood was not modulated in any interpretable manner, the author believes that these results suggest that vitamin/mineral supplementation has the potential to improve brain function in healthy children, and warrant further investigation. (7)
716 girls who enrolled at four Baltimore high schools were screened for non-anaemic iron deficiency (serum ferritin < or = 12 micrograms/L with normal haemoglobin). 98 (13.7%) girls had non-anaemic iron deficiency of whom 81 were enrolled in the trial.
Participants were randomly assigned oral ferrous sulphate (650 mg twice daily) or placebo for 8 weeks. The effect of iron treatment was assessed by questionnaires and haematological and cognitive tests, which were done before treatment started and repeated after the intervention. We used four tests of attention and memory to measure cognitive functioning. Intention-to-treat and per-protocol analyses were done.
Of the 81 enrolled girls with non-anaemic iron deficiency, 78 (96%) completed the study (39 in each group). Five girls (three control, two treatment) developed anaemia during the intervention and were excluded from the analyses. Thus, 73 girls were included in the per-protocol analysis. Ethnic distribution, mean age, serum ferritin concentrations, haemoglobin concentrations, and cognitive test scores of the groups did not differ significantly at baseline. Postintervention haematological measures of iron status were significantly improved in the treatment group (serum ferritin 27.3 vs 12.1 micrograms/L, p < 0.001).
Regression analysis showed that girls who received iron performed better on a test of verbal learning and memory than girls in the control group (p < 0.02). (8)
Low levels of vitamin D were associated with an increased risk of high blood pressure, high blood sugar and metabolic syndrome in teenagers, researchers reported at the American Heart Association’s 49th Annual Conference on Cardiovascular Disease Epidemiology and Prevention.
In the study, researchers analyzed 3,577 adolescents, 12 to 19 years old (51 percent boys), who participated in the nationally representative National Health and Nutrition Examination Survey (NHANES) conducted in 2001–2004.
After adjusting for age, sex, race/ethnicity, body mass index, socioeconomic status and physical activity, researchers found the adolescents with the lowest levels of vitamin D were:
• 2.36 times more likely to have high blood pressure;
• 2.54 times more likely to have high blood sugar; and
• 3.99 times more likely to have metabolic syndrome.
Metabolic syndrome is a cluster of cardiovascular disease and diabetes risk factors including elevated waist circumference, high blood pressure, elevated triglycerides, low levels of high-density lipoprotein (HDL or “good”) cholesterol and high fasting glucose levels. The presence of three or more of the factors increases a person’s risk of developing diabetes and cardiovascular disease.
Low levels of vitamin D are strongly associated with overweight and abdominal obesity. (9)
Catherine M. Gordon, M.D., M.Sc., and colleagues at Children's Hospital Boston, studied 380 healthy children ages 8 months to 24 months who visited a primary care center for a physical examination between 2005 and 2007. Parents filled out a questionnaire regarding their nutritional intake and that of their children, and also reported on the use of vitamin D and other supplements, time spent outdoors, socioeconomic status and education level.
Among the 365 children for whom blood samples were available, 12.1 percent (44) had vitamin D deficiency, defined as 20 nanograms per milliliter of blood or less, and 40 percent (146) had levels below the accepted optimal level of 30 nanograms per milliliter. Breastfed infants who did not receive vitamin D and toddlers who drank less milk were at higher risk of deficiency (for each cup of milk toddlers drank per day, blood vitamin D level increased by 2.9 nanograms per milliliter).
Forty children of the 44 with vitamin D deficiency underwent X-rays of the wrist and knee. Thirteen (32.5 percent) had evidence of bone mineral loss, and three (7.5 percent) exhibited changes to their bones suggestive of rickets.
The data suggest that infants should receive vitamin D supplements while breastfeeding and raise the question of whether some children, including those with established risk factors for vitamin D deficiency, should receive regular measurements of blood vitamin D levels. (10)
Pneumonia is a leading cause of morbidity and mortality in young children.
In a double-blind placebo-controlled clinical trial in Matlab Hospital, Bangladesh, 270 children aged 2-23 months were randomized to receive elemental zinc (20 mg per day) or placebo, plus the hospital's standard antimicrobial management, until discharge.
The outcomes were time to cessation of severe pneumonia (no chest indrawing, respiratory rate 50 per min or less, oxygen saturation at least 95% on room air) and discharge from hospital. Discharge was allowed when respiratory rate was 40 per minute or less for 24 consecutive hours while patients were maintained only on oral antibiotics.
The group receiving zinc had reduced duration of severe pneumonia (relative hazard [RH]=0.70, 95% CI 0.51-0.98), including duration of chest indrawing (0.80, 0.61-1.05), respiratory rate more than 50 per min (0.74, 0.57-0.98), and hypoxia (0.79, 0.61-1.04), and overall hospital duration (0.75, 0.57-0.99). The mean reduction is equivalent to 1 hospital day for both severe pneumonia and time in hospital. All effects were greater when children with wheezing were omitted from the analysis.
Adjuvant treatment with 20 mg zinc per day accelerates recovery from severe pneumonia in children. (11)
OBJECTIVES: Folate and the metabolically related B vitamins are an important priority throughout life, but few studies have examined their status through childhood and adolescence.
The aims of the current study were to investigate age, gender, and lifestyle factors as determinants of folate, related B-vitamin status, and homocysteine concentrations among British children and adolescents and to propose age-specific reference ranges for these biomarkers, which, at present, are unavailable.
PARTICIPANTS AND METHODS: Data from the National Dietary and Nutritional Survey of 2127 young people aged 4 to 18 years were accessed to provide a representative sample of British children.
All of the subjects who provided a blood sample for homocysteine concentrations were included in the current study (n = 840). Of these, laboratory biomarkers of folate (serum and red cell folate: n = 832 and 774, respectively), vitamin B(12) (n = 828), vitamin B(6) (n = 770), and riboflavin (n = 839) were also examined.
RESULTS: The biomarker status of all 4 of the relevant B vitamins decreased significantly with age. Correspondingly, homocysteine concentrations progressively increased, with median values of 5.6, 6.3, and 7.9 mumol/L for children aged 4 to 10 years, 11 to 14 years, and 15 to 18 years, respectively, and were higher in boys compared with girls (15-18 years only). Independent of age and gender, fortified breakfast cereal intake (consumed by 89% of the sample) was associated with significantly higher B-vitamin status and lower homocysteine concentrations. (12)
1. Singh M. Role of micronutrients for physical growth and mental development. Indian J Pediatr. 2004 Jan;71(1):59-62.
2. Bull World Health Organ vol.82 no.3 Genebra Mar. 2004.
3. Huh S, Gordon C. Vitamin D Deficiency in children and Adolescents: Epidemiology, impact and treatment. Rev Endocr Metab Disord (2008) :(161-170).
4. Gordon C, Feldman H, Sinclair L et al. Prevalence of Vitamin D deficiency among healthy infants and toddlers: Archives Pediatrics and Adolescent Medicine 2008:162(6):505-512.
5. Garland C, Garland F, Gorham E, Lipkin M et al. The Role of Vitamin D in Cancer Prevention. American Journal of Public Health 2006 February: Vol 96(2) 252-261.
6. Stahl A, Vohmann C, Richter A, Heseker H, Mensink GB. Changes in food and nutrient intake of 6- to 17-year-old Germans between the 1980s and 2006. Public Health Nutr. 2009 Feb 23:1-12. [Epub ahead of print]
7. Haskell Crystal F; Scholey Andrew B; Jackson Philippa A; Elliott Jade M; Defeyter Margaret A; Greer Joanna; Robertson Bernadette C; Buchanan Tom; Tiplady Brian; Kennedy David OCognitive and mood effects in healthy children during 12 weeks' supplementation with multi-vitamin/minerals. British Journal of Nutrition. 100(5):1086-96, 2008 Nov
8. Bruner AB, Joffe A, Duggan AK, Casella JF, Brandt J. Randomised study of cognitive effects of iron supplementation in non-anaemic iron-deficient adolescent girls. Lancet. 1996 Oct 12;348(9033):973.
9. Reis JP, von Muhlen D, Miller III ER, et al. Vitamin D status and cardiovascular disease risk factors in the us adolescent population. AHA 49th Annual Conference on Cardiovascular Disease Epidemiology and Prevention; March 11, 2009; Palm Harbor, FL. Poster P54.
10. Catherine M. Gordon; Henry A. Feldman; Linda Sinclair; Avery LeBoff Williams; Paul K. Kleinman; Jeannette Perez-Rossello; Joanne E. Cox. Prevalence of Vitamin D Deficiency Among Healthy Infants and Toddlers. Arch Pediatr Adolesc Med., 2008;162(6):505-512
11. Brooks WA, Yunus M, Santosham M, Wahed MA, Nahar K, Yeasmin S, Black RE. Zinc for severe pneumonia in very young children: double-blind placebo-controlled trial. Lancet. 2004 May 22;363(9422):1683-8
12. Kerr MA, Livingstone B, Bates CJ, Bradbury I, Scott JM, Ward M, Pentieva K, Mansoor MA, McNulty H. Folate, related B vitamins, and homocysteine in childhood and adolescence: potential implications for disease risk in later life. Pediatrics. 2009 Feb;123(2):627-35.